AT the dawn of a year and decade, it is fitting to review and renew our goals. 2020 holds special meaning for everyone who appreciates the sense of sight and especially for me as an eye specialist. “20/20 vision” is medical parlance for normal or optimal visual sharpness: what a healthy eye should be able to see clearly, at 20 feet. “Vision 2020: The Right to Sight” is also the name of a World Health Organization (WHO) project that was launched in 1999 as part of an ongoing project commenced 30 years ago, with the aim of eliminating avoidable blindness globally by 2020.
A global guidance and blueprint for eye care systems, Vision 2020 started with advocacy for intervention against eye diseases such as cataract, glaucoma, diabetes, Vitamin A deficiency and trachoma (parasitic river blindness prevalent in Africa) as its first priorities. To sum up Vision 2020, WHO published its comprehensive World Report on Vision last year, freely available on the Internet. Although unmet needs still exist, the project has seen unprecedented progress and is deemed successful by most yardsticks. There has been a very significant reduction in cases of eye infections and blindness from Vitamin A deficiency, as well as the ongoing reduction in prevalence of blindness among adults, including treatable causes.
Nevertheless, continuous focus is necessary as these results can’t keep pace with the growth of an ageing population. The report includes the global magnitude of the issues, successes, what remains to be done, recommended strategies and paths charted for the future. The causes of vision impairment and their impact on financial burden are of particular interest to me. The figures are staggering: at least 2.2 billion people have vision impairment globally. At least one billion of these (an underestimation according to the report) could have been prevented or are unaddressed, with 123.7 million suffering from unaddressed refractive errors.
Cataract comes in second at 65.2 million. These eye conditions are projected to increase due to population ageing, as well as environmental and lifestyle changes. From the report, the cost of the coverage gap for global unaddressed refractive errors and cataract was estimated to be US$14.3 billion. In the world, there are an estimated 2.6 billion people with myopia (of which 312 million are under 19 years old) and 1.8 billion with presbyopia. These contributed to losses in annual global productivity estimated to be US$244 billion and US$25.4 billion, respectively. The prevalence of myopia is the highest in East, South and Southeast Asia. It was reported in these regions that the economic burden of uncorrected myopia was more than double that of other regions and equivalent to one per cent of gross domestic product (GDP).
A simple calculation should convince one of the highly cost-effective outcomes for addressing treatment of myopia, presbyopia and cataract – my three main areas of practice in ophthalmology – in any health care system. There are several points in the report that strike a pertinent yet sensitive note. First, the issue of funding for management of the commonest eye condition, that is, refractive errors, which in many countries are mostly out-of pocket. These include the costs of spectacles, deemed an assistive device, as well as contact lenses and refractive surgeries such as LASIK. Second, the potential role for public-private partnerships to improve eye care services. What is new for this decade is the focus of “integrated people-centred eye care” as a continuum of health intervention.
This is a new addition to the WHO project’s action plan to now include integration of eye care into health care systems, ideally across all sectors, and, for this, four important strategies are proposed. These are to empower and engage people and communities, reorientate model of care, coordinate services within and across sectors, and create an enabling environment. In my mind, these are applicable to both policymakers and the public. Integration of eye care into health care is here to stay. For the general public, it should translate to ensuring good eye care and visual habits from the groundup, starting in the family, schools, public institutions, at work and at leisure.
It also means having eye protection in sports and in relevant occupations and attending eye screenings regularly even when the eyes feel fine, as some eye diseases are silent in the initial stages where they can be controlled and potentially reversed. Ensuring good general health and lifestyle is key in maintaining good eye health. Our eye clinic also welcomes the new decade with an addition of the services provided. Incorporating a Refractive and Cataract Surgery service on site has long been our aim. We look forward to deliver safe, effective and integrated eye care with the addition of the trusted Johnson and Johnson Star S4 iLASIK excimer laser with FDA approved wavefront guided treatment via its latest iDesign 2.0 and the Swiss-made Ziemer Z8 femtolaser for OCT-guided thin flap LASIK surgery, being the first in Singapore, as well as for laser cataract surgery.
These will help address the most common eye conditions in the world – namely myopia, presbyopia and cataract – in an efficient and affordable manner.
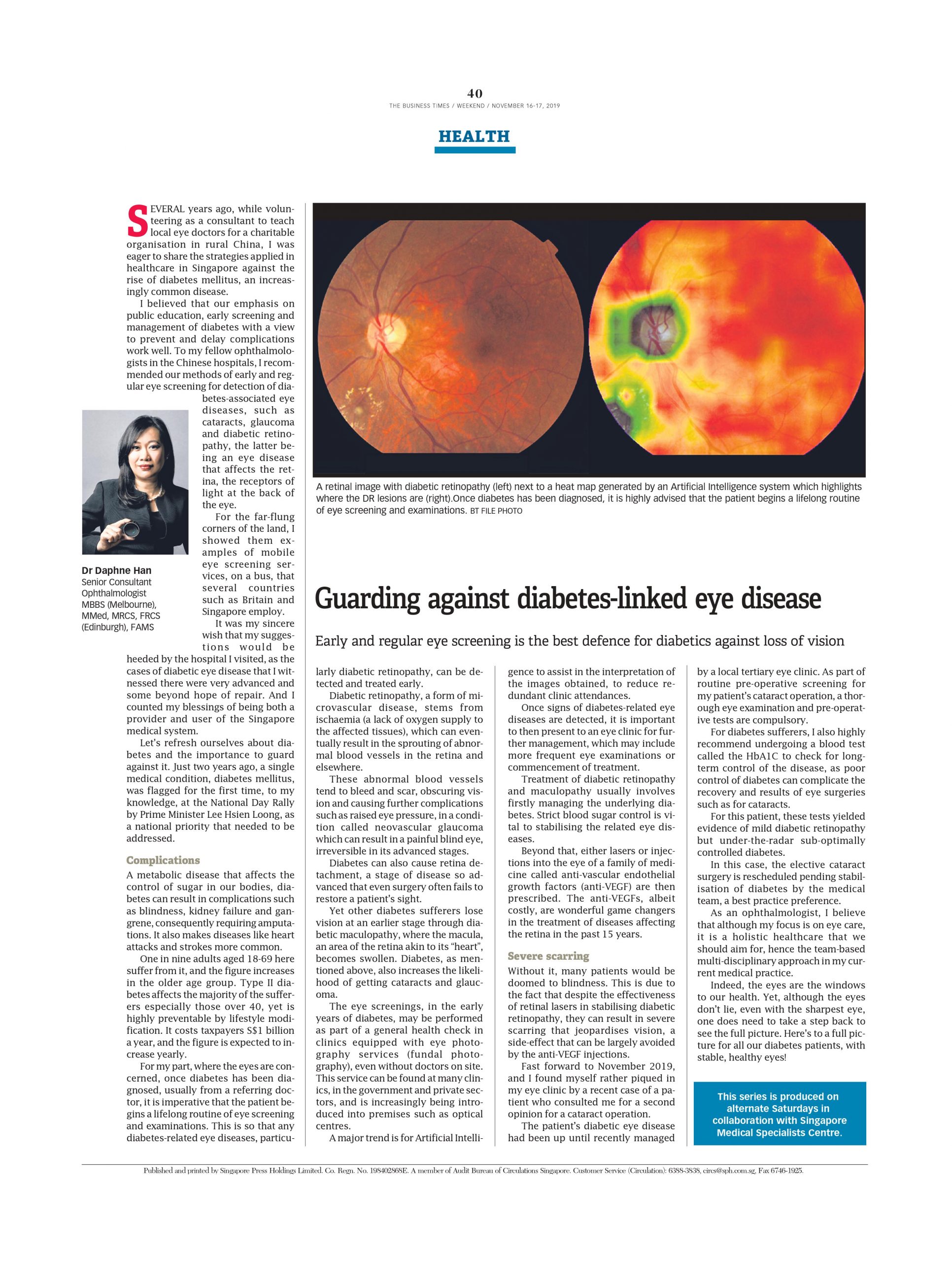
The Ziemer Z8 also looks forward to providing further innovations in flapless refractive lenticule treatment for myopia in the near future. Eye screening enabled with artificial intelligence for front-of-eye diseases by dual-Scheimpflug imaging and back-of-eye diseases by digital angiography and fundal camera remains our go-to option, a sign of the times.
Dr Daphne Han
Senior Consultant Ophthalmologist
MBBS (Melbourne), MMed, MRCS, FRCS (Edinburgh), FAMS
THE BUSINESS TIMES WEEKEND JANUARY 11, 2020