TREADMILL testing is a common modality used by many doctors to screen for heart artery disease. For the couch potatoes who are suddenly fired up to become a paragon of fitness, current guidelines recommend that it will be wise for relatively inactive older men to undergo a treadmill stress test before embarking on a vigorous exercise regime. If the treadmill test result appears normal, does that mean that you do not have heart artery disease and you will not get a heart attack? If the test result is abnormal, does it mean that you have significant heart artery disease?
What is a treadmill stress test?
The treadmill stress test, though a commonly used screening test by doctors, has many limitations, especially for women. Patients are hooked up to a monitor which records the electrical pattern of the heart – also known as an electrocardiogram (ECG) – and walk on a treadmill machine which increases in speed and incline every few minutes according to the preset protocol. During the test, doctors look for changes in the ECG to screen for heart artery disease.
Treadmill test in women
Research from the last decade has revealed gender differences in heart disease. American Heart Association statistics have shown that 64 per cent of women who died suddenly from heart disease did not have classic warning symptoms, versus 50 per cent of men.
Moreover, 38 per cent of women died within one year following a heart attack, versus 25 per cent of men. Hence, there is a need to detect underlying heart artery disease in women. Although treadmill testing is widely used, the pitfalls of this method need to be understood.
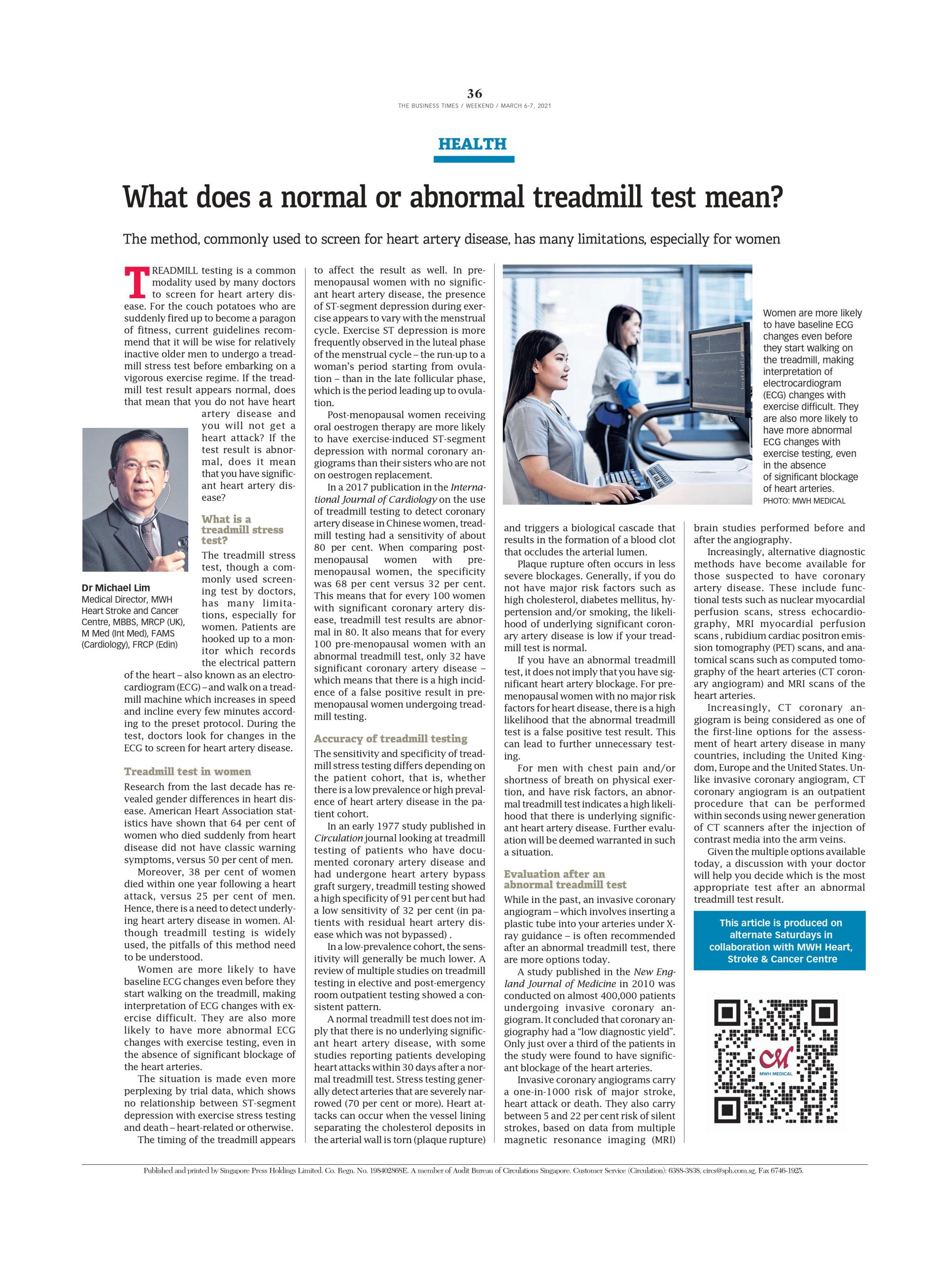
Women are more likely to have baseline ECG changes even before they start walking on the treadmill, making interpretation of ECG changes with exercise difficult. They are also more likely to have more abnormal ECG changes with exercise testing, even in the absence of significant blockage of the heart arteries.
The situation is made even more perplexing by trial data, which shows no relationship between ST-segment depression with exercise stress testing and death – heart-related or otherwise.
The timing of the treadmill appears to affect the result as well. In pre-menopausal women with no significant heart artery disease, the presence of ST-segment depression during exercise appears to vary with the menstrual cycle. Exercise ST depression is more frequently observed in the luteal phase of the menstrual cycle – the run-up to a woman’s period starting from ovulation – than in the late follicular phase, which is the period leading up to ovulation.
Post-menopausal women receiving oral oestrogen therapy are more likely to have exercise-induced ST-segment depression with normal coronary angiograms than their sisters who are not on oestrogen replacement.
In a 2017 publication in the International Journal of Cardiology on the use of treadmill testing to detect coronary artery disease in Chinese women, treadmill testing had a sensitivity of about 80 per cent. When comparing post-menopausal women with pre-menopausal women, the specificity was 68 per cent versus 32 per cent. This means that for every 100 women with significant coronary artery disease, treadmill test results are abnormal in 80. It also means that for every 100 pre-menopausal women with an abnormal treadmill test, only 32 have significant coronary artery disease – which means that there is a high incidence of a false positive result in pre-menopausal women undergoing treadmill testing.
Accuracy of treadmill testing
The sensitivity and specificity of treadmill stress testing differs depending on the patient cohort, that is, whether there is a low prevalence or high prevalence of heart artery disease in the patient cohort.
In an early 1977 study published in Circulation journal looking at treadmill testing of patients who have documented coronary artery disease and had undergone heart artery bypass graft surgery, treadmill testing showed a high specificity of 91 per cent but had a low sensitivity of 32 per cent (in patients with residual heart artery disease which was not bypassed) .
In a low-prevalence cohort, the sensitivity will generally be much lower. A review of multiple studies on treadmill testing in elective and post-emergency room outpatient testing showed a consistent pattern.
A normal treadmill test does not imply that there is no underlying significant heart artery disease, with some studies reporting patients developing heart attacks within 30 days after a normal treadmill test. Stress testing generally detect arteries that are severely narrowed (70 per cent or more). Heart attacks can occur when the vessel lining separating the cholesterol deposits in the arterial wall is torn (plaque rupture) and triggers a biological cascade that results in the formation of a blood clot that occludes the arterial lumen.
Plaque rupture often occurs in less severe blockages. Generally, if you do not have major risk factors such as high cholesterol, diabetes mellitus, hypertension and/or smoking, the likelihood of underlying significant coronary artery disease is low if your treadmill test is normal.
If you have an abnormal treadmill test, it does not imply that you have significant heart artery blockage. For pre-menopausal women with no major risk factors for heart disease, there is a high likelihood that the abnormal treadmill test is a false positive test result. This can lead to further unnecessary testing.
For men with chest pain and/or shortness of breath on physical exertion, and have risk factors, an abnormal treadmill test indicates a high likelihood that there is underlying significant heart artery disease. Further evaluation will be deemed warranted in such a situation.
Evaluation after an abnormal treadmill test
While in the past, an invasive coronary angiogram – which involves inserting a plastic tube into your arteries under X-ray guidance – is often recommended after an abnormal treadmill test, there are more options today.
A study published in the New England Journal of Medicine in 2010 was conducted on almost 400,000 patients undergoing invasive coronary angiogram. It concluded that coronary angiography had a “low diagnostic yield”. Only just over a third of the patients in the study were found to have significant blockage of the heart arteries.
Invasive coronary angiograms carry a one-in-1000 risk of major stroke, heart attack or death. They also carry between 5 and 22 per cent risk of silent strokes, based on data from multiple magnetic resonance imaging (MRI) brain studies performed before and after the angiography.
Increasingly, alternative diagnostic methods have become available for those suspected to have coronary artery disease. These include functional tests such as nuclear myocardial perfusion scans, stress echocardiography, MRI myocardial perfusion scans , rubidium cardiac positron emission tomography (PET) scans, and anatomical scans such as computed tomography of the heart arteries (CT coronary angiogram) and MRI scans of the heart arteries.
Increasingly, CT coronary angiogram is being considered as one of the first-line options for the assessment of heart artery disease in many countries, including the United Kingdom, Europe and the United States. Unlike invasive coronary angiogram, CT coronary angiogram is an outpatient procedure that can be performed within seconds using newer generation of CT scanners after the injection of contrast media into the arm veins.
Given the multiple options available today, a discussion with your doctor will help you decide which is the most appropriate test after an abnormal treadmill test result.








